

ROTATOR CUFF STRAIN VS TEAR: YOUR COMPLETE GUIDE
TL;DR: Rotator Cuff Strain vs Tear
Key Difference: Strain = overstretched/frayed muscle-tendon fibres (milder); Tear = partial/full rupture of tendon (more severe).
Symptoms:
- Strain: Dull ache after activity, mild weakness/stiffness, improves with rest (2-12 weeks).
- Tear: Sharp pain (often sudden/pop), night pain, significant weakness (can’t lift arm), clicking.
Causes: Both from overuse/trauma; tears more from age (>50), smoking, impingement.
Diagnosis: Exam + ultrasound/MRI for tears; X-ray rules out bone issues.
Treatment: 80%+ non-surgical (rest, PEACE & LOVE protocol, physio); surgery for large/traumatic tears.
Red Flags (see doc ASAP): Sudden weakness, can’t lift arm, no improvement in 1-2 weeks.
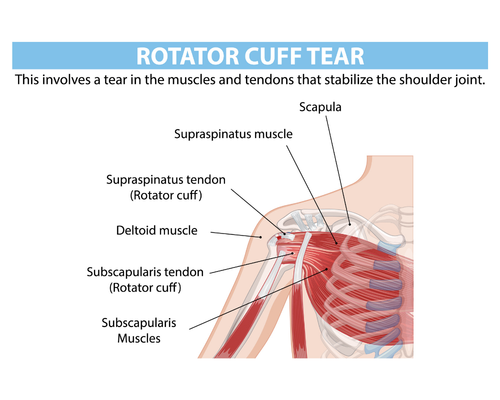
What is The Rotator Cuff?
The rotator cuff is a group of four muscles and their tendons (supraspinatus, infraspinatus, teres minor, subscapularis) that stabilise your shoulder and allow you to lift and rotate your arm. These muscles connect the shoulder blade to the top of the arm bone (humerus) and keep the ball of the shoulder centred in the socket during movement.
Common causes of rotator cuff problems include repetitive overhead work, sports such as tennis, swimming, cricket and baseball, falls, and age‑related wear and tear. Rotator cuff injuries are especially common after age 30-40 and are a leading cause of persistent shoulder pain and weakness.
Rotator Cuff Strain vs Tear: The Key Difference
A rotator cuff strain is an overstretching or microscopic damage of the muscles and tendons without complete disruption of the tissue. It is usually caused by sudden overload or repetitive overuse and is considered a “milder” injury on the spectrum.
A rotator cuff tear occurs when the tendon actually separates from the bone or is significantly disrupted, and it can be partial‑thickness (only part of the tendon involved) or full‑thickness (the tendon is torn through its full depth, sometimes fully detached). Tears can develop suddenly after trauma (acute tears) or slowly over time from degeneration and impingement.
Simple Way to Think About it
- Strain: like overstretching a rope so some fibres are frayed, but the rope is still in one piece and working.
- Tear: the rope has a deeper cut or is completely snapped, so strength and function are more clearly affected.
Grading: How Bad is The Strain or Tear?
Many clinicians describe rotator cuff injuries on a three‑grade scale that covers both strains and tears.
| Grade | What it means (tendon/muscle) | Typical function |
|---|---|---|
| Grade 1 | Mild stretching with microscopic fibre damage; tendon or muscle remains structurally intact. | Sore and stiff but usually able to use the arm; pain often settles with relative rest and guided rehab. |
| Grade 2 | More substantial fibre damage, like a “frayed rope” or partial tear; overall continuity is still present. | Noticeable weakness and more painful movement; overhead or heavier activity may be limited or uncomfortable. |
| Grade 3 | Full‑thickness or complete rupture of the tendon or muscle. | Marked weakness with difficulty or inability to lift the arm; typically requires assessment by a specialist. |

Rotator Cuff Strain vs Tear: Symptoms
Strains and tears can share symptoms, but some red flags point more toward a significant tear.
Rotato Cuff Strain Symptoms
Typical rotator cuff strain symptoms can include:
- Dull, aching pain around the top or side of the shoulder, often after activity.
- Pain with lifting, reaching overhead, or rotating the arm, but usually manageable.
- Mild weakness or fatigue in the shoulder muscles.
- Stiffness, especially after rest or first thing in the morning.
- Pain that generally improves with rest and activity modification over days to weeks.
Rotato Cuff Tear Symptoms
Typical rotator cuff tear symptoms can include:
- Sharp or more intense pain at the time of injury, sometimes with a popping or tearing sensation.
- Persistent pain that worsens with lifting or lowering the arm and when lying on the affected side at night.
- Noticeable weakness. Difficulty raising the arm overhead, reaching behind your back, or lifting everyday objects.
- Crackling, grinding or clicking (crepitus) with shoulder movement.
- In full‑thickness tears, it may be impossible to lift the arm above shoulder height or away from the body.
Some rotator cuff tears cause little or no pain, especially degenerative tears in older adults, and may be found incidentally on MRI. Pain intensity alone does not reliably indicate how bad the structural damage is.
Rotator Cuff Strain vs Tear: Causes and Risk Factors
Shared Causes
Both rotator cuff strains and tears can result from:
- Repetitive overhead movements (painting, manual trades, racquet sports, swimming).
- Sudden overload, such as lifting something heavy or awkward, or a fall onto an outstretched arm.
- Poor shoulder posture and mechanics, especially slouched posture and impingement.
Tear Specific Risk Factors
- Ageing: tendon quality declines with age; degenerative tears are very common after 50.
- Smoking: linked to more frequent and more severe rotator cuff tears.
- Long history of overhead sport or labour, especially without adequate conditioning.
- Previous partial tears or long‑standing impingement syndrome.
How to Tell: Rotator Cuff Strain or Tear
You cannot be 100% sure without an assessment, but these patterns help guide suspicion.
Features More Suggestive of a Strain
- Gradual onset of pain after increasing training, DIY or workload.
- Discomfort rather than severe pain at rest; movement is sore but still possible.
- Weakness is mild, more like “tiredness” than sa udden loss of strength.
- Symptoms start to ease with a few days of rest and simple home care.
Features More Suggestive of a Tear
- Sudden, sharp pain at the moment of injury, often with a “snap” or “pop”.
- Immediate or rapid loss of strength. Struggling to lift the arm or hold objects.
- Night pain that keeps you awake, especially lying on that shoulder.
- Symptoms that persist or worsen beyond one to two weeks despite rest.
Because shoulder sprains (ligaments) can mimic rotator cuff tears, and both can coexist, a thorough clinical exam is essential rather than relying purely on self‑diagnosis.
Diagnosis: How Clinicians Assess Rotator Cuff Strains & Tears
A good assessment usually combines history, physical tests, and sometimes imaging.
1. Clinical History & Physical Examination
Your clinician will ask about:
- How the pain started (sudden trauma vs gradual overload).
- Exact location of pain (top of shoulder, outer arm, front of shoulder).
- Activities or positions that aggravate or ease pain.
- Night pain, weakness, clicking and any sense of instability.
They will then test shoulder range of motion, strength of individual cuff muscles, and perform special tests that tension specific tendons and look for impingement.
2. Imaging: When & Why
Your clinician will ask about:
- How the pain started (sudden trauma vs gradual overload).
- Exact location of pain (top of shoulder, outer arm, front of shoulder).
- Activities or positions that aggravate or ease pain.
- Night pain, weakness, clicking and any sense of instability.
They will then test shoulder range of motion, strength of individual cuff muscles, and perform special tests that tension specific tendons and look for impingement.
Treatment For Rotator Cuff Strains vs Tears
Treatment overlaps significantly, especially early on, but severity and goals drive the plan.
Conservative (non-surgical) Care; First-Line For Most Injuries
Around 80–85% of people with rotator cuff injuries improve with non‑surgical treatment. This typically includes:
- Relative rest and activity modification: avoiding or reducing overhead and heavy lifting while staying generally active.
- PEACE & LOVE protocol.
- Structured physiotherapy and exercise physiology: targeted strengthening of rotator cuff and scapular stabilisers, mobility work and gradual load progression.
- Posture and movement re‑education to reduce impingement and mechanical overload.
- Corticosteroid injection: sometimes used for persistent pain to calm inflammation and allow rehab to progress.
Physiotherapy is central for both strains and many tears and often allows patients to avoid or delay surgery.
When is Surgical Treatment For Rotator Cuff Injuries Considered?
Surgery is usually reserved for:
- Large or full‑thickness tears with significant functional loss.
- Acute traumatic tears in younger or highly active patients.
- Symptoms persisting 6-12 months despite high‑quality non‑surgical care.
Common surgical options include arthroscopic tendon repair, open repair for complex or massive tears, tendon transfer, or reverse total shoulder replacement in severe, irreparable cases with arthritis. Surgical recovery involves a period in a sling (often 4-6 weeks) followed by months of progressive physiotherapy, with many people regaining good function by about 4-6 months.
Recovery Time: Strain vs Tear
Recovery time depends on injury grade, your age, general health and how well you follow rehab.
- Mild strain (Grade 1): often improves over 2-4 weeks with appropriate rest and exercises.
- Moderate strain/partial‑thickness tear: commonly requires 8-12 weeks or more of structured rehab to restore strength and function.
- Full‑thickness tear managed conservatively: may improve symptomatically over months but residual weakness can remain.
- Post‑surgical repair: sling for up to 4-6 weeks, then progressive rehab over several months; full strength and range can take 4-6 months or longer.
Tendon healing is slow because of relatively poor blood supply, so even with ideal management, you should expect “good days and bad days” rather than linear improvement.

Self Care Tips for Suspected Rotator Cuff Strain
If your symptoms sound more like a mild to moderate strain and there are no red flags (see below), simple measures can help.
- Reduce overhead and heavy lifting for a few weeks rather than complete rest.
- Start gentle pain‑free range‑of‑motion exercises (pendulums, supported forward reach) and progress to light strengthening when pain allows.
- Prioritise posture – avoid prolonged slumping at a desk and adjust workstations where possible.
If pain is not clearly improving after 1–2 weeks, or if you rely on pain medication to cope with everyday tasks, you should seek professional assessment.
When to See a Physiotherapist or Doctor Urgently
Seek prompt medical or physiotherapy review if:
- You had a fall or sudden injury with immediate sharp pain and loss of strength.
- You cannot lift or rotate your arm as you normally would.
- You notice visible deformity, significant swelling or bruising around the shoulder.
- Night pain is severe or worsening and interrupts sleep regularly.
- Symptoms have not improved after 1–2 weeks of rest and simple care.
Early assessment and targeted treatment help prevent minor strains from progressing and improve outcomes for more significant tears.
Rotator Cuff Strain vs Tear: Quick Comparison
| Feature | Rotator cuff strain | Rotator cuff tear |
|---|---|---|
| Definition | Overstretching or micro-damage of muscle or tendon without full disruption. | Partial or full-thickness disruption of the tendon, sometimes fully detached from bone. |
| Onset | Often gradual after overuse or sudden increase in activity. | Sudden after trauma or progressive with age-related degeneration and impingement. |
| Pain pattern | Dull ache, activity-related, improves with rest. | Sharper, more intense; night pain is common and may not settle with rest. |
| Weakness | Mild, feels more like fatigue. | Noticeable weakness, difficulty or inability to lift arm overhead. |
| Imaging findings | May be normal; shows inflammation or minor fibre changes if present. | Partial or full-thickness tear visible on ultrasound/MRI. |
| Typical treatment | Non-surgical: activity modification, ice, medication, physiotherapy. | Usually starts non-surgically; larger or traumatic tears may need surgical repair plus rehab. |
| Recovery time | Often 2-12 weeks depending on severity. | Months for full recovery; surgery adds 4-6 months of structured rehab. |
In summary, rotator cuff strain vs tear differs mainly in severity. Strains involve overstretching with milder pain and quicker recovery (2–12 weeks), while tears cause significant weakness, night pain, and may need surgery after failed physio. We’ve covered symptoms, causes, diagnosis (exam/ultrasound/MRI), treatments, and red flags like the inability to lift your arm. For accurate assessment and tailored physiotherapy in Sydney’s Burwood, Top Ryde, Newington, or East Gardens clinics, book today to prevent progression and restore shoulder function.


